
We don’t know how to treat this Doctors and patients in Russia are fighting for coronavirus drugs that hardly help anyone
In early September, more than one million Russians were battling the coronavirus. Statistics show that many regions are now in the midst of experiencing a second wave. However, no one seems to know how to treat the virus effectively as of yet. “Meduza” special correspondent Svetlana Reiter and science editor Alexander Ershov investigate the different drugs being used to treat the coronavirus in Russia and find out who’s profiting during the pandemic.
The fight for medications
“While working in Russia, we got used to everything, but it was a shock. At the peak of the pandemic in the regions, our distributors were told openly: don’t ship us enough covid medications, you can forget about our market — we’ll squeeze you out,” a source from Sanofi, one of the world’s largest pharmaceutical companies, told Meduza.
In the spring of 2020, Russia’s negotiations on drug procurement were tense. A Meduza source recalls that Moscow and the Moscow Region were the first to “get a move on with the applications for medications,” but in other regions it was “chaos”: suppliers no longer had the required amount of drugs and the local authorities were besieging distributors. As a result, pharmaceutical companies had to cut corners to provide for everyone — they say so themselves.
The main battle unfolded over the anti-malaria drug hydroxychloroquine — at the pandemic’s peak it was considered the main medication for COVID-19. “We agreed on emergency deliveries from Europe to our warehouse within a month — the logistics service managed to push everything through barely working customs during quarantine,” Meduza’s source from Sanofi explains. “While the cargo was moving, our distributors muddled along as best they could, [saying] we’ll give you less now and more later, the pandemic won’t be limited to one month, you’ll need more later.”
The doctors Meduza interviewed from various Russian regions confirmed these claims. “There were problems at the beginning: there were no medicines,” recalls a doctor from a hospital in Barnaul (Altai Krai), who spoke on condition of anonymity. According to infectious disease specialist Saniyat Magomedova, an associate professor at Dagestan State Medical University (DGMU), “The leadership tried to get [medications] but were unsuccessful” — apparently a commission from Moscow determined that since mortality rates in Dagestan were low, they “didn’t require anything extra.”
Patients’ relatives ended up purchasing medications at their own expense — there were even shortages of the most basic antibiotic, azithromycin (used to treat a variety of bacterial infections, including pneumonia), a doctor from St. Petersburg’s Alexandrovskaya Hospital told Meduza, on condition of anonymity.
“Everyone knew that the coronavirus was somewhere out there, in China, and then in Europe. [But] in actual fact no one in Russia was ready for this,” Meduza’s source from Sanofi recalls. “[Coronavirus] medication piled up at one hospital, but the neighboring one had none, one clinic doesn’t share with the other. Colleagues from other pharmaceutical companies whose relatives were hospitalized wrote to us and asked us to give them a chance to buy something at least.”
But at the peak of the pandemic, no one knew that the medicines they so desperately wanted — and which were in such limited supply — wouldn’t actually cure them of the virus. There’s no cure even now, though everyone is waiting for one.
The problem with hydroxychloroquine
Forty-year-old top manager Egor contracted the coronavirus infection at the end of April. It started with a fever: the first day his temperature hit 37.5 degrees Celsius (99.5 degrees Fahrenheit), by day four it rose to 39 degrees Celsius (102.2 degrees Fahrenheit) and didn’t come down.
Initially, Egor thought it was just a cold — he drank tea with honey and lemon. When the home remedies didn’t work, he went for a chest x-ray and CT scan, which revealed bilateral pneumonia. “They sent me home from the hospital and told me to call a doctor. I called for an ambulance all evening,” Egor recalls. Eventually, he was sent to a private hospital that had been reprofiled to treat coronavirus patients.
Egor spent more than two weeks in the hospital, during which his treatment plan was changed three times. The medical reports he shared with Meduza show that he was initially treated with broad-spectrum antibiotics, as well as vitamins and cough syrup. When this failed to bring down his fever, Egor, on the recommendation of his brother, asked the doctors to prescribe hydroxychloroquine — a medication originally developed to prevent and treat malaria, rheumatoid arthritis, and lupus.
“[My brother] said: ‘Insist as much as possible that they give it to you.’ At that moment it was the most fashionable medication for ‘corona.’ I told the doctor about it: ‘My brother recommends it, maybe, you’ll try it?’ And they started to give me hydroxychloroquine,” Egor recalls.
Hydroxychloroquine is an antimalarial drug with potential antiviral effects. Chloroquine, hydroxychloroquine, and mefloquine are all similar medications. These drugs penetrate intracellular vesicles (endosomes) and change their pH level, which is supposed to stop most viruses from reproducing (including COVID-19 and SARS). However, this only works in vitro (in other words, in a test tube).
The antiviral potential of antimalarial drugs was known before the pandemic. Hydroxychloroquine’s popularity for treating COVID-19 arose in March. An article by French virologist Didier Raoult describes the reduction of viral loads in patients who took hydroxychloroquine in conjunction with Azithromycin. While the study is questionable given its small sample size (36 people), the low cost, availability, lack of alternatives, and encouraging preliminary data led to hydroxychloroquine’s inclusion in the WHO-initiated Solidarity Trial and many other clinical trials.
We now know that antimalarial drugs have dangerous side effects and don’t reduce time spent in the hospital or the fatality rate. As such, several hydroxychloroquine studies were stopped ahead of schedule and the FDA revoked permission to use hydroxychloroquine to treat COVID-19. In early July, the WHO excluded it from the Solidarity Trial.
Neither the US National Institute of Health (NIH) nor the WHO suggest chloroquine and hydroxychloroquine for treating COVID-19 or similar illnesses.
The Russian Health Ministry first mentioned chloroquine in its temporary methodological guidelines on March 27, and it remains there to this day. The latest version, published in early September, mentions that antimalarial drugs are excluded from WHO trials. However, the authors insist that foreign studies and domestic experience indicate the possible effective use of hydroxychloroquine in small doses in patients with mild and moderate forms of COVID-19.
Hydroxychloroquine comes with a long list of side effects, which includes diarrhea, heart failure, psychosis, and suicidal behavior. In conversation with Meduza, a nurse from a coronavirus hospital in Nizhny Novgorod recalled a patient who experienced muscle antony (the medical term for loss of strength) after taking the drug: “Not just weakness, like many people, rather, she just couldn’t get up.”
In Egor’s case, his blood pressure spiked. He took the new medication for six days, but his temperature didn’t drop. The doctors took him off hydroxychloroquine and put him back on antibiotics. “They told me honestly: ‘Basically, we don’t know how to treat you. [It’s like] we’re shooting sparrows with a cannon — maybe, we’ll hit one’,” Egor recalls. Nevertheless, in the end he recovered: the doctors concluded that his body had beaten the infection on its own.
“We started working [with it] in April, the Health Ministry had just approved the guidelines for using hydroxychloroquine as an antiviral agent. There were works that showed that it could be effective — weak evidence, but nothing else,” explains Darya Kamyshova, a clinical pharmacologist from Moscow’s Pirogov Center. According to her, treating patients with hydroxychloroquine yielded few visible results; when research data later revealed that “the drug was most likely ineffective” she “wasn’t surprised.” But not everyone at her hospital was willing to give up on medication right away. “It’s difficult for a doctor to resist the desire to treat, even if essentially there aren’t any suitable medications,” she says.
Update. According to Yuri Mochalin, Sanofi’s director of corporate relations in Eurasia, the company saw a surge in demand for hydroxychloroquine in the first half of this year, due to publications that spoke to “the drug’s potential antiviral effects on COVID-19.” In response, “the company decided to prioritize patients according to registered indications,” he told Meduza. In other words, patients with a medically valid reason for using this drug — not COVID-19 patients specifically. When Russia’s regional health authorities requested hydroxychloroquine — to be used as a treatment for the coronavirus — the company supplied it “as an exception.” Mochalin made these comments to Meduza after the original publication of this article in Russian (available here).
The price of guidelines
Despite conflicting clinical research, hydroxychloroquine remains listed in the Russian Health Ministry’s clinical guidelines. The ministry has also recommended mefloquine — along with some other drugs — for treating COVID-19.
“The pandemic, the frenzy, the incredible expectation in the search for some kind of panacea that can save us all. It’s clear that this was happening all over the world [...] But in Russia we were facing the fact that those government institutions that should act as a buffer between the manufacturers and the consumers, essentially assume the functions of advertising agencies and introduce whatever they like into the methodological guidelines,” says Svetlana Zavidova, a representative of the Association of Clinical Research Organizations, with outrage.
As Zavidova points out, mefloquine is produced by the Federal Biomedical Agency’s (FMBA) company Khimzashchita. It was included in the Health Ministry’s guidelines up until the beginning of September, but it’s not in the latest version.
FMBA director and former health minister Veronika Skvortsova has repeatedly referred to mefloquine as an effective treatment for COVID-19. “It completely suppresses the virus in 48 hours and reduces its effects by 75 percent when taken preventatively,” she said in May.
Meanwhile, hospitals purchased 7.6 million rubles (more than $97,000) worth of mefloquine from February to April of this year. And more than 236,000 ($3,000) rubles were spent on it at pharmacies. For comparison, the DSM Group estimated (at Meduza’s request) that 10,000 rubles (less than $130) were spent on the purchase of mefloquine in 2019.
“The drug is old, heavy, and has side effects, but in Russia it is used actively [to treat] malaria. And the FMBA got the idea that it needed to be added to the guidelines for treating covid — along with hydroxychloroquine, which has similar effects. You have to understand that we, as an association, never get involved in treatment issues. But here we even wrote to the Health Ministry, because we couldn’t stand it: on April 10, the FMBA published a loud statement that they had proven the antiviral properties of mefloquine against the COVID-19 pathogen. It turned out that they meant the laboratory tests and the effects of the drug on cell cultures in vitro,” Zavidova explains.
Meduza spoke to several doctors from Moscow and other regions about the use of this drug. On condition of anonymity, doctors from Barnaul, Krasnodar, St. Petersburg, and Nizhny Novgorod told Meduza they’ve never used mefloquine to treat COVID-19. It wasn’t used very actively in Moscow hospitals either.
Asked about mefloquine, clinical pharmacologist Darya Kamyshova tells Meduza that her hospital has never used it to treat the coronavirus, adding that using it seems like a “dubious idea.” On top of the lack of research on the drugs effects on COVID-19, Kamyshova warns of its range of side effects, “including the development of serious neurological disorders.” The chief physicians from two of Moscow’s main coronavirus hospitals — the O.M. Filatov Hospital and the I.V. Davidovsky Hospital — also confirmed that they aren’t using mefloquine to treat patients with COVID-19.
FMBA spokeswoman Anna Sprogis didn’t respond to Meduza’s questions when contacted via messenger.
Treatment and bureaucracy
Meduza’s source at Sanofi says that at the beginning of the pandemic, the drug procurement process was slowed down due to the fact that the medications being used to treat COVID-19 were registered for other diseases. As a work around, hospitals had the relevant departments sign the procurement bids based on the drugs in question. For example, rheumatologists signed orders for tocilizumab, a drug meant to treat rheumatoid arthritis, even though doctors intended to use it to treat severe coronavirus cases, recall two Meduza sources from pharmaceutical companies.
“At the beginning, hospitals purchased according to the illness indicated on the instructions, otherwise these purchases wouldn’t have been paid for. Then they started working according to the new regulations,” Meduza’s source close to the Health Ministry’s leadership explains.
In late March, the Finance Ministry simplified procurement procedures. But in the regions, things didn’t get any easier. “They told us that Moscow holds the strategic reserve,” recalls researcher Saniyat Magomedova from Dagestan State Medical University. “If this decision had been made earlier, people without tocilizumab wouldn’t have died from [hyperinflammation],” Meduza’s source at Sanofi insists.
There were no such shortages in the capital: Marina Lysenko, the chief physician at Moscow City Clinical Hospital Number 52, says tocilizumab showed some results in treating severe cases of COVID-19; despite the fact that clinical studies say otherwise.
Tocilizumab is an antibody that binds to the receptor and inhibits the activity of interleukin-6 (one of the signaling molecules that promotes inflammation processes that play an important role in severe cases of COVID-19). It seemed like a promising treatment for COVID-19 based on experience using it to treat similar illnesses involving immune system hyperactivation. That said, the drug didn’t significantly lower fatalities rates in clinical trials.
NIH guidelines clearly advise against using tocilizumab or its analogs. However, Russian guidelines pay a lot of attention to it, recommending the drug as a treatment for extensive lung lesions resulting from acute respiratory distress syndrome (ARDS) — one of the main complications arising from COVID-19.
“Since COVID-19 came to Russia later than China and Italy, we already had their valuable experience, it was easier for us. For example, in Moscow, [hyperinflammation] blockers were included in the treatment protocols at the majority of clinics immediately. We administered tocilizumab widely and early, at the first signs of hyperinflammation. In many patients, the clinical effects were undeniable,” insists Elena Vasilyeva, the chief physician at Moscow’s I. V. Davydov Hospital.
As of July 8, local clinics have been required by government order to treat patients according to Health Ministry guidelines. As a doctor from St. Petersburg tells Meduza (on condition of anonymity), the federal healthcare watchdog, Roszdravnadzor, and the Federal Compulsory Medical Insurance Fund are demanding exact compliance with these rules, “including all the [antiviral drugs] thrown in there.”
In Russia, clinical guidelines are usually written by a medical organization (for example, the Pediatrician’s Union of Russia or the Russian Cardiologists’ Society). However, unlike typical clinical recommendations, the Health Ministry’s “Temporary Methodological Recommendations” for treating COVID-19 patients aren’t just medical. Although these types of guidelines aren’t considered legally binding, the temporary guidelines for treating the coronavirus were made mandatory as of July 8, 2020.
Russia is also set to change the status of clinical guidelines in general; as of January 1, 2022, medical care must be given “on the basis of clinical guidelines” and this will be the first thing taken into account when Roszdravnadzor evaluates the quality of treatment. This decision has generated great controversy in Russia, since it’s not uncommon to find statements contained in Russian clinical guidelines that contradict modern medical science.
Legally, patients have the right to refuse treatment, but since the coronavirus is considered a danger to others, COVID-19 patients aren’t allowed to refuse treatment entirely. That said, since there are several treatment options included in the Health Ministry’s guidelines, a doctor is unlikely to be considered in violation of the law if they refrain from using a particular drug. And, according to doctors, this is exactly what some of them are doing.
When 45-year-old journalist Ilyas was being treated for the coronavirus, along with his mother, doctors had them sign consent forms for “experimental treatment,” after which they were prescribed azithromycin and hydroxychloroquine. His mother experienced high blood pressure and breathing problems, and was hospitalized for two weeks. TV host Pavel Lobkov says that when he came down with the coronavirus, “the doctors at the clinic gave me all sorts of medications right away.” They prescribed him “both Kaletra and hydroxychloroquine.” His neighbor, Denis Protsenko — the chief physician at Moscow’s main coronavirus hospital in Kommunarka — told him not to drink and to look out for breathing problems.
Doctors actively used the antiviral drug sold under the brand name Kaletra (lopinavir/ritonavir) at the start of the pandemic, but according to clinical pharmacologist Darya Kamyshova, they didn’t see any noticeable effects. “In our hospital, we didn’t include Kaletra and hydroxychloroquine in [our] protocol, because in my opinion it was already clear in April that there was no evidence of the benefits of these drugs, and there were many side effects,” adds Dr. Elena Vasilyeva. Nevertheless, Kaletra was included in the Health Ministry guidelines from April until September (it has since been removed). Vasilyeva says its a pity hydroxychloroquine is still included.
Kaletra, a well-known AIDS drug, is a combination of the protease inhibitors lopinavir and ritonavir. Based on experiments on animals infected with the coronavirus species known as Middle East Respiratory Syndrome (MERS), it seemed like this combination of inhibitors might effectively treat COVID-19. However, the drug failed in a small but reputable study. Kaltera didn’t show any antiviral effects in subsequent trials, but did cause a number of side effects, including diarrhea, nausea, vomiting, migraines, and increased blood pressure. NIH experts don’t recommend using the drug to treat COVID-19.
We’re all equal in the face of the virus
Doctor Vasily Kupreichik specializes in rehabilitation. In April, he was working in the emergency room at N.I. Pirogov Hospital in Moscow. His first shift was on April 17 — four days later, all of the places reserved for coronavirus patients were full. At first, they mainly used Kaletra, hydroxychloroquine, and antibiotics to treat COVID-19 patients, Kupreichik explains. “At some point the emphasis began to shift, and I noticed [that] incoming patients had a tendency towards thrombosis [blood clots], and we needed to deal with thrombosis prevention, and not give out Kaletra for no reason,” he recalls. “[It] has zero benefit, but many side effects. I wrote about it on Facebook.”

After a brief stint in the hospital’s intensive care unit — where Kupreichik says “people work like machines” — he left to work as a consultant for “anyone high-end.” In other words, he’s now providing medical care for wealthy people.
However, it turns out that they aren’t getting much more than the standard treatment. Meduza obtained a list of treatments used on the mayor of a regional capital in southern Russia. When he fell ill with the coronavirus in July (there were no official reports), he was prescribed Kaletra immediately.
Speaking anonymously, an assistant to an oligarch living in Europe (one included in the Forbes top-100 , tells Meduza that everyone hoped money could save them. But it quickly became clear that there was no set treatment — no one knew what to buy. “The boss bought paracetamol and a couple packages of hydroxychloroquine — it seems he didn’t even open them. I tried to reserve a room at the hospital, but they refused him,” the assistant explains, adding that his boss was initially under the impression that he could buy a ventilator to use at home, but quickly realized the device would be useless without a specialist to operate it.
Russian officials and businesspeople have tried anything and everything to escape from COVID-19. One of Russia’s top businessmen reserved a room in a private clinic and kept the intensive care unit to himself for the entirety of the lockdown, to the tune of several million rubles (hospital employees and an outside doctor familiar with the hospital’s leadership confirmed this for Meduza, on condition of anonymity).
Many wealthy people, including Mark Garber, senior partner at the wealth management company GHP Group, sought treatment at the Lapino Clinic, which is owned by famous obstetrician-gynecologist Mark Kurster (who is also a business partner of Rostec CEO Sergey Chemezov).
Garber told Meduza that when he contracted COVID-19 in March, he was treated with Kaletra, then hydroxychloroquine, antibiotics, azithromycin, as well as vitamins C, D, and zinc. He also took anti-anxiety medication “because antimalarial drugs can cause depression and even suicide.”
Billionaire Dmitry Bosov, who committed suicide in early May, was taking hydroxychloroquine daily to prevent COVID-19, two of his close friends told Meduza. His widow declined our request for comment, stating “I will not comment on the life of my family.”
Russia’s response to America’s remedy
According to doctor Yaroslav Ashikhimin, his wealthy clients are willing to shell out $10,000 for a box of remdesivir — an American antiviral drug considered the main pharmacological weapon against COVID-19. When clients told him they were willing to pay thousands of dollars for the medication, he had to explain to them that its effectiveness is still questionable.
A study showed that remdesivir only worked in the early stages of the virus, either before or when a patient starts to experience respiratory failure. Because people in the early stages of the disease rarely go to the hospital, most patients in intensive care aren’t treated with this drug. Nevertheless, the American government bought out almost the entire supply of remdesivir (brand name, Veklury) from its manufacturer, Gilead Sciences.

Remdesivir is a nucleotide analog synthesized by the American biopharmaceutical company Gilead Sciences and studied as an inhibitor of RNA virus reproduction. It affects the RNA polymerase of viruses, causing it to make mistakes, and thereby suppressing its reproduction. It works on a wide spectrum of viruses including Ebola, Nipah, SARS-CoV-1, and MERS.
Virology experts had high hopes for remdesivir, primarily because the drug has a clear and specific mechanism of action. However, its injectable form isn’t suitable for preventative use. Data from some studies shows that remdesivir promotes faster recovery (an average of 11 days compared to 15 days among the placebo group), but the resulting decrease in mortality wasn’t significant enough to prove its effects.
NIH guidelines cautiously recommend using remdesivir for patients with severe cases of the virus who require oxygen support but aren’t on a ventilator. American experts don’t have enough reliable arguments for or against its use in mild and moderate cases. Broader studies on the benefit-risk ratio are needed.
Clinical studies on the drug began in Russia over the summer. The Roche Company, in cooperation with Gilead Sciences, is currently conducting a study on the effects of treating COVID-19 with a combination of remdesivir and tocilizumab. Meanwhile, the Russian pharmaceutical company Pharmasyntez is also conducting a study on Russia’s first generic form of remdesivir, called Remdeform.
Pharmasyntez, which produces Kaletra for HIV treatment, has seen a significant increase in turnover during the pandemic — from February to June inclusively, the company signed contracts worth about two billion rubles (nearly $26 million). According to estimates from the DSM Group, the figures from the same period in 2019 were one and half times lower. In conversation with Meduza, Pharmasyntez founder Viram Punia speaks of the company’s financial performance with pride: its turnover, which was one billion rubles in 2010, has now reached 30 billion rubles (about $388 million).
Pharmasyntez created its generic form of remdesivir back in February. Twenty-three Russian clinics are participating in the clinical trials for Remdeform. The study involves a total of 220 patients, all of whom had “moderately severe” cases of COVID-19 and allegedly recovered in a week instead of the standard two. Since the results of the study haven’t been published as of yet, these claims cannot be verified.
Mass production of remdesivir is supposed to start in October or November. Pharmasyntez founder Vikram Punia plans to ask the government for a compulsory license so that Pharmasyntez can produce Remdesivir without permission from Gilead Sciences (the latter owns the patent for the original medication until at least 2031. According to Punia, “Pharmasyntez has repeatedly approached Gilead Sciences with an offer to pay royalties amounting to 2 percent on sales in exchange for a voluntary license,” but has yet to receive a response).
That said, there’s other competition coming from within Russia. R-Pharm — one of the largest suppliers of drugs recommended by the Health Ministry for treating COVID-19 — has created its own generic version of remdesivir, as well. “We’re finished with mice and will now conduct a clinical trial with people,” R-Pharm board chairman Alexey Repik told Meduza.
The St. Petersburg-based pharmaceutical company Aktivny Komponent (Acticomp) is also planning to produce remdesivir. According to company president Alexander Semynov, Acticomp started developing the drug back in March, “in case it were to be in demand in the fall because of a new wave of the pandemic.”
The Japanese option
“Avifavir helped us a lot, people started getting discharged not in three weeks, but after a week,” a municipal official from one of Russia’s central regions told Meduza.
The official was referring to the antiviral medication favipiravir, which is sold in Russia under the nowwell-known brand names Avifavir and Coronavir. These generic versions were developed by the Russian pharmaceutical companies R-Pharm and ChemRar. Doctors in Japan tried treating coronavirus patients with another brand name version, Avigan, but had little success.
Favipiravir is a nucleotide analog with a mechanism similar to remdesivir. Both can inhibit the RNA polymerase of several viruses in vitro. Favipiravir is produced as a tablet (which is an advantage), but it’s significantly less studied than remdesivir.
Little was known about the drug at the start of the pandemic. As with remdesivir, studies were conducted in vitro. Even before the epidemic, the substance had potential as a broad-spectrum antiviral agent — first and foremost as a flu medication.
Like Russia, Japan, China, and India are also interested in favipiravir. The US, Great Britain, and other countries aren’t because of the lack of reliable data. One Chinese study that compared favipiravir with lopinavir/ritonavir (without randomization) observed a reduction in the viral load. But overall the same problems arose as with remdesivir, which were further complicated by the significant lack of data. While it’s possible that the drug really does suppress the reproduction of the virus, it still isn’t clear if this could decrease mortality.
The FDA recently approved a Phase II of a study of favipiravir (meant to compare the drug’s safety and effectiveness), but NIH guidelines don’t mention favipiravir at all. In April, the WHO considered including favipiravir in its Solidarity Trial, but never made a decision.
In Russia’s guidelines, favipiravir occupied a central place among all the antiviral drugs. The results of the above-mentioned Chinese study and a similar study in Russia are presented as arguments in favor of its use.
The Russian Health Ministry added favipiravir to its treatment guidelines in June. Before that, it approved clinical trials of R-Pharm’s Koronovir and Kromis’s Avifavir (a joint venture between ChemRar and the Russian Direct Investment Fund). The fund invested actively in businesses related to the coronavirus, ranging from tests for the virus to the vaccine developed by the Gamaleya Research Institute. The head of the Russian Direct Investment Fund, Kirill Dmitriev, postponed interviews with Meduza twice and never ended up speaking with us.

Kromis told Meduza that it conducted clinical trials for Avifavir involving 30,00 patients in 51 regions and later issued an interim report. The company said the drug helps suppress the disease in its early stages and prevents progression to more severe stages. A Kromis representative added that Chinese doctors tried “several dozen drugs” for treating the coronavirus, but by mid-March had only expressed confidence in the effectiveness of “one drug” — favipiravir.
Chief physicians at the Russian hospitals conducting the clinical trials for favipiravir had differing opinions. Maryana Lysenko from Moscow City Clinical Hospital Number 52 praises the drug, saying they observed a “clear decrease in viral load” among their patients (according to her, this was during a clinical trial involving 20 participants and an observational study involving 60). But Valery Vechorko from the Filatov Clinical Hospital believes it’s too early to take a position: “there patients who recover [after] taking favipiravir, and there are patients who we had to take off the drug [due to] increased liver enzymes,” he explains.
Clinical pharmacologist Darya Kamyshova agrees: “By the time favipiravir came out, I was far more cautious about anything without proven effectiveness. And there are no studies available with a good evidence base in favor of the drug. It’s difficult to draw conclusions based on our experience,” she says. While some of the patients at the Pirogov Center showed signs of improvement, others had bad reactions to the drug.
R-Pharm board chairman Alexey Repik told Meduza that he “killed the coronavirus in three days using favipiravir.” Repik — who ranks 49th on the Forbes billionaires list, with an estimated fortune of $1.2 billion — diagnosed himself with the coronavirus in June, took favipiravir, and conducted his own tests (also on his own initiative). He claims the viral load had “completely disappeared” by the fourth day. Regardless of its many side effects, Repik considers favipiravir the “drug of choice for outpatient treatment,” because it allows you to catch the disease “at the earliest moment.” Previously, favipiravir was only used in hospitals — the Health Ministry cleared it for outpatient use as of September 17 and it was expected to hit pharmacies by September 21.
The Russian versions of favipiravir — Koronavir, Avifavir, and Areplivir — were featured in a powerful ad campaign, in which the media announced the “first effective Russian drugs for COVID” — a study from Fujita University spoiled it; the scientists there said that favipiravir doesn’t help treat the coronavirus. ChemRar dismissed the study and, along with the Russian Direct Investment Fund, began large-scale deliveries of the favipiravir to Brazil.
According to government procurement data, Russia’s hospitals have already spent 367 million rubles (about $4.8 million) on favipiravir. “We personally sold 17,000 packages for 12,000 rubles each. We made about 200 million rubles,” Repik recalls (that’s about $2.6 million in total, with each package selling for about $155).
That said, Repik insists that pharmaceutical companies aren’t making major profits from coronavirus drugs: “At the beginning of September, we earned about a billion rubles [$13 million] from coronavirus medications. At the same time, the volume of investment in these drugs — in development, clinical research, manufacturing — is five to seven billion rubles [$65–91 million],” he says.
Old friends
According to estimates from the DSM Group, requested by Meduza, more than 10 billion rubles (more than $130 million) were spent on coronavirus medications at Russia’s hospitals and pharmacies from February to June, inclusively.
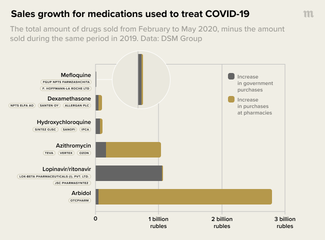
During that same period, nearly four billion rubles (about $52,000) were spent on the antiviral drug Arbidol (umifenovir) at pharmacies alone — four times more money than was spent on it in 2019. The drug’s Russian manufacturer, OCTPharm, was formerly part of Pharmstandard — the pharmaceutical company behind the fortune of Russian billionaire Viktor Kharitonin (who is, in turn, a longtime acquaintance of Deputy Prime Minister Tatyana Golikova, the head of the federal headquarters for the fight against the coronavirus).
Despite the fact that Russia’s Federal Antimonopoly Service deemed advertising Arbidol as a cure for COVID-19 illegal — on top of the fact that it isn’t a registered drug in the US and the WHO has omitted it from its guidelines for treating the flu — the drug’s sales have only gone up. And it’s included in all of the Russian Health Ministry’s guidelines, so it’s being given out to coronavirus patients at local clinics and handed out by doctors making house calls.
The Russian biopharmaceutical company Nanolek is also involved in manufacturing drugs to treat COVID-19. The company’s president, Vladimir Khristenko, is the son of former Minister of Industry Viktor Khristenko, who is married to Deputy Prime Minister Golikova. Khristenko junior also used to work for Pharmstandard.
In May, Nanolek registered a generic form of hydroxychloroquine — the first batch was released at a plant in Kirov in June. Russia’s largest hydroxychloroquine manufacturer, Biocom (which is owned by the conglomerate Sistema and the state corporation Rostec), registered Nanolek as an additional manufacturer of the drug. A Biocom representative told Meduza that this was a precaution, taken “to provide the country with the necessary amount of the drug in case the COVID-19 situations worsens.”
The representative added that before the pandemic, Biocom was producing up to 4,000 packages of hydroxychloroquine per year; between the start of the pandemic and April 2020, the production volume increased to 170,000 packages.
The Second Wave
Denis Protsenko, the chief physician at Moscow’s main COVID-19 hospital in Kommunarka, promised that there wouldn’t be a second wave in Russia, but the country remains fourth in the world for the highest number of coronavirus cases. On October 9, the country registered more than 12,000 new cases of COVID-19.
“We never reached zero, but in the middle of the summer we had less than 100 patients [with the coronavirus at the same time], but now it’s 200,” explains infectious disease researcher Saniyat Magomedova from Dagestan Medical University. The hospital where she works as a consultant has started favoring Dexamethasone — a corticosteroid medication that’s readily available, inexpensive, and supposedly helps reduce hyper-inflammation.
Dexamethasone is an anti-inflammatory steroid, one of many similar drugs including prednisone and methylprednisolone. It’s main use in COVID-19 treatment is to prevent the development of systemic inflammation.
Little was known about Dexamethasone at the beginning of the pandemic. Corticosteroids were mentioned in passing as a means to combat Acute Respiratory Distress Syndrome (ARDS), but doctors didn’t have high hopes.
Dexamethasone was the first drug able to significantly decrease the fatality rate for COVID-19 — by about a third. This happened on June 16, and since then, the encouraging results of the first trial have generally only been confirmed.
NIH experts recommend only using the drug for those who need oxygen support. There are no proven benefits for those that don’t. The Russian guidelines are similar, but they maintain that the drug should be prescribed in response to signs of immune system hyperactivation, rather than based on blood oxygen saturation.
Like the rest of Russia, Moscow is seeing a growing number of coronavirus patients. In September, the Russian capital was recording about 700 new cases daily. On October 9, it registered 3,700 new cases of COVID-19.
Valery Vechorko, chief physician at Moscow’s O. M. Filatov Clinical Hospital, recently tested positive for coronavirus antibodies; he was taking hydroxychloroquine regularly as a preventative measure. Clinical pharmacologist Daria Kamyshova from the Pirogov Center also fell ill. She told Meduza that she had mild symptoms, a severe headache and a fever — she maintains that she treated it with “normal ice cream” and nothing else.
Maryana Lysenko, chief physician at City Clinical Hospital Number 52, believes doctors have learned how to deal with the complications from the virus, though they still can’t kill it in its earliest stages. “You want us to tell you how to cure coronavirus — at the same time, you want it to be one pill, so that we can learn to live with this virus. But that’s not going to happen […] until there’s collective immunity, only a vaccine can help,” she maintains. However, the vaccine won’t be widely available in Russia until February 2021, and that’s the best case scenario. And so long as there’s no vaccine, doctors will go on treating patients with whatever they have.
Story by Svetlana Reiter and Alexander Ershov, with additional reporting by Pavel Merzlikin, Ivan Golunov, Daria Sarkisyan, and Farida Rustamova.
Edited by Tatyana Lysova
Translated and abridged by Megan Luttrell and Eilish Hart